Herding Cats

It has been repeated ad nauseam that “working in healthcare IT is like herding cats“, a refrence to the challenges to faced in change management of Clinicians and other supporting actors in the provision of care. In their paper “Herding Cats: The Challenges of EMR Vendor Selection [1]”. Doctors McDowell & Michelson remind us that in the case of migrating to an EMR;
“In some instances, the process may represent only an incremental change in a partially developed computerised EMR. In other cases, it comes closer to a revolution, as it is part of a complete overhaul of a minimally computerised medical record system. In the latter circumstance, the implementation of the EMR involves much more than simply automation of preexisting processes. Strategically it requires analysis of, and change to, the underlying clinical information processes.”
In other words, it requires a change to the actual practise of care and naturally there will be resistance from your clinicians. Which is why the authors rather cheekily allude to the herding of cats in their title.
The Value of Information

Fundamental to the practise of medicine is the medical record. The practise has evolved to codify knowledge, track patients as individuals, part of a cohort or on an epidemiological scale and track studies and research before the information revolution – so the question is often set up wrongly,as “do we need to go paperless?”. The real question should be how much faster, more collaborative, more comprehensive, more accessible simultaneously and more persistent and available do we need our medical record to be? Popular culture is saturated enough by IT for all to understand the value of information through software, so while everyone looks looking up information on a computer and the added benefits of analytics it affords, many dislike the disruptive nature of the EMR is making providers change their workflows, be more disciplined with documentation and having to do things in certain methodologies or process steps. Resistance then often comes not from a hatred of screens or keyboards but the intrusivenes of having someone else dictate your methodology and process.
Rethinking our Change Management Strategy

The conventional wisdom is usually to engage clinicians at the very begining and then buy some monolithic application that does everything from billing claims to medical records and struggle with integration to the myriad of anxilliary life science software that already exist such as medical imaging, pharmacy management & laboratory systems. What ends up happening is either a paralysis of choosing a system or a fallout from Clinicians who lost the vote and then provide resistance to the change that the chosen software will bring to their work.
I have from my experience adopted a different approach. Let me give you a high level overview to get you thinking;
0. Build a decent IT department with real IT experts because no matter what you choose, the fundamentals underlying everything is IT.
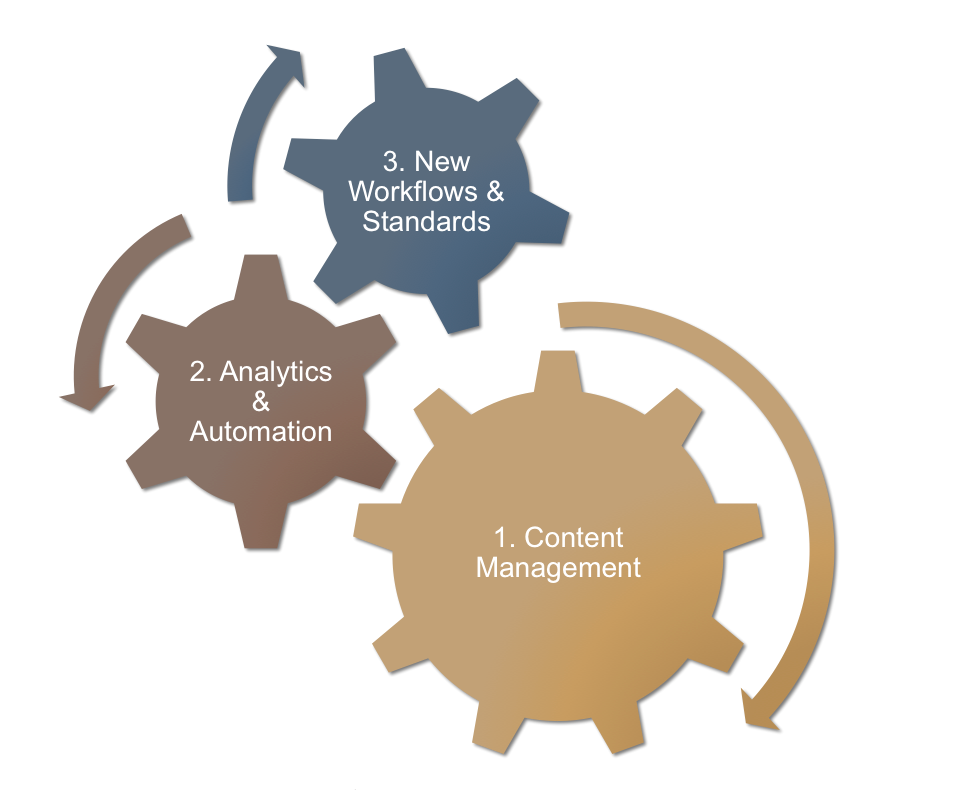
1. The Content Management Phase. Let those experts work on a data integration strategy – how to build a complete 360 view of a patient, from operational, financial and medicine that the different stakeholders can use at the point of need to access all the information they need about the patient their attending to. This will involve the digitisation of legacy records, from scanned images, to Optical Character Recognition and patching in existing digital information that already exist. What they will end up building is a digitisation bureau and a data warehouse that will be able to provide a consolidated patient record to any application you choose to use later.
2. The Analytics & Automation Phase. Avoid talking about new workflows and process, rather begin by providing Clinicians and Operational staff more and more access to patient centered information at their convenience on their computers and mobile devices in a secure and reliable fashion. Quickly churn out analytics from this data warehouse such as some basic measures of outcomes, productivity or even commercial insights such as revenue drivers, performing departments and efficiency of different support services.
3. The New Workflows & Standards Phase. Only change the method of input and data capture with new workflows and tools after steps 1 to 3 are established. The added benefit of having completed step 1 is that you now have a bigger selection of applications that can be used since all of them tap the record from the common data warehouse. Many experienced healthcare people reading this now will protest that this can’t be done, but honestly if step 0 is done correctly, we won’t need to have this debate.
———————————–
[1] “Herding Cats: The Challenges of EMR Vendor Selection” by Samuel W. McDowell, PhD, Regi Wahl, and James Michelson, MD in the Journal of Healthcare Information Management — Vol. 17, No. 3
